PRIAPISM - AN INTERESTING ULTRASOUND CASE
A 35 year old male patient came with chief complaints of continuous painful erection of penis for last 6 days.There is no history of any trauma, drug intake or any haematological disorders.
| . :   |
| Clinical examination revealed fully erect penis |
On ultrasound Doppler evaluation
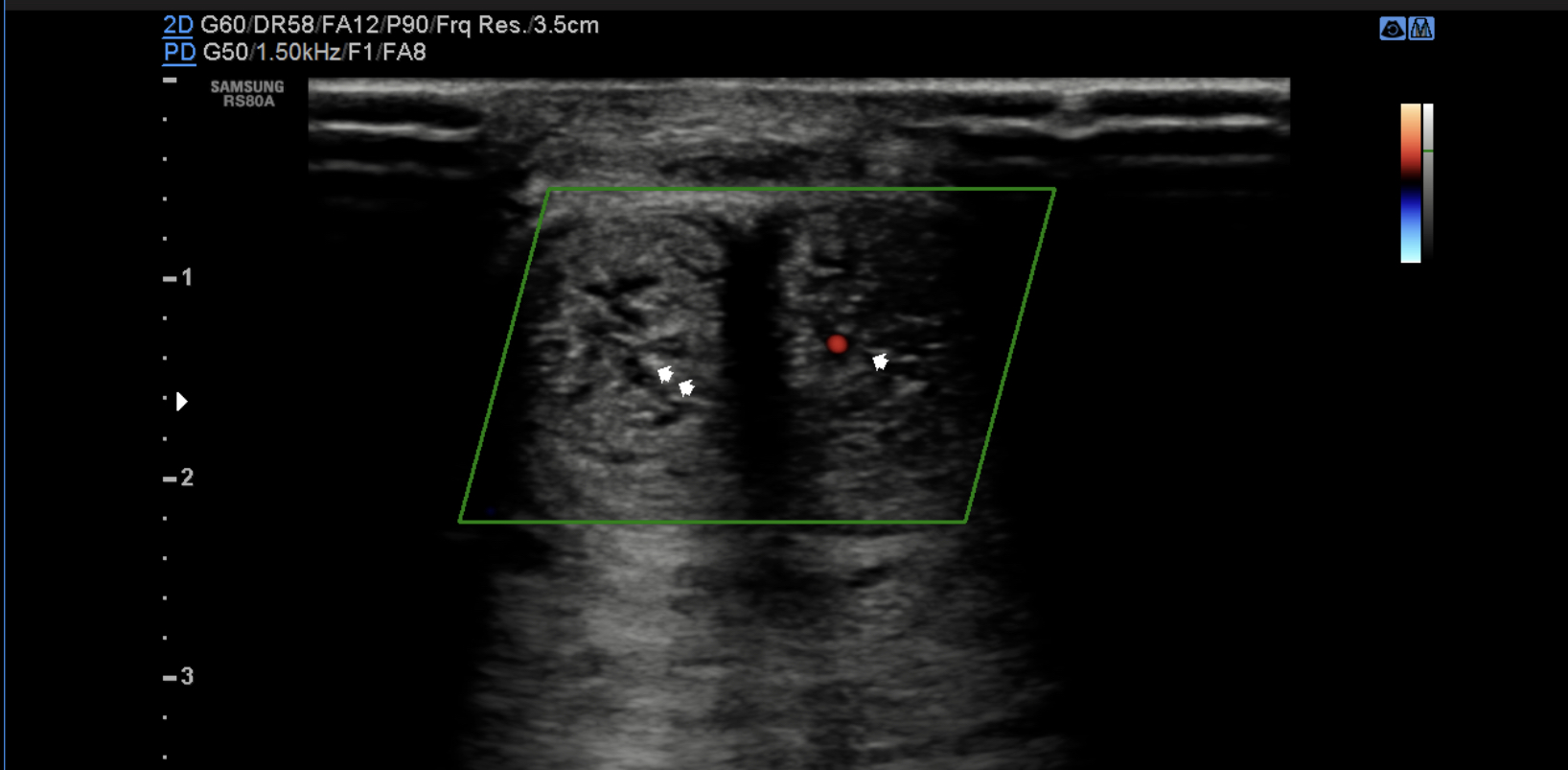 |
Transverse image through the engorged penile shaft shows absent flow in the right cavernosal artery(double arrow), the left cavernosal artery shows vascularity (single arrow) but decreased flow  Decreased peak systolic velocity noted in left cavernosal artery Decreased peak systolic velocity noted in left cavernosal artery Priapism Priapism is defined as a penile erection that persists for 4 h or longer and is unrelated to sexual activity. It can be of three types
 Anatomy  UltrasoundPurpose is to differentiate high and low velocity priapism. Cavernosal blood flow will be typical absent or there will be a low velocity high resistance flow in low flow type as shown below  In some cases of ischaemic priapism, high arterial flow is still present but the reversal of diastolic flow (indicative of high-resistance) and the absence of fistula can differentiate these cases from non-ischaemic priapism as shown below  Non-ischaemic priapism is normally associated with high PSV, low- resistance flow and the presence of turbulent flow from fistula.  MriThe penis should be secured with tape to the anterior abdominal wall. Thin-section (4 mm or less) high-resolution images are necessary with a small field of view. Intravenous contrast is essential to demonstrate cavernosal perfusion and help predict areas of necrosis. T1 - high T1 intensity thrombus can be demonstrated. T2 - can demonstrate flow voids in high flow type Cavernosal blood gas analysisIschaemic type - hypoxic, hypercarbic and acidotic Non ischaemic type - normal Treatment |
Aspiration of corporal blood +/- intracorporal injection of detumescent agents (phenylephrine). In refractory cases decompression with a shunt is required in order to preserve penile length - for ischaemic type
Internal pudendal arteriography with selective catheterization and embolisation is the gold-standard treatment. The fistulae can self resolve and conservative management is therefore sometimes appropriate.
Corporal aspiration and medical therapy should be avoided. - for non ischaemic types.


Informative and precise
ReplyDelete